
ADRENAL Crisis
Adrenal crisis and severe acute adrenocortical insufficiency are often elusive diagnoses that may result in severe morbidity and mortality when undiagnosed or ineffectively treated.
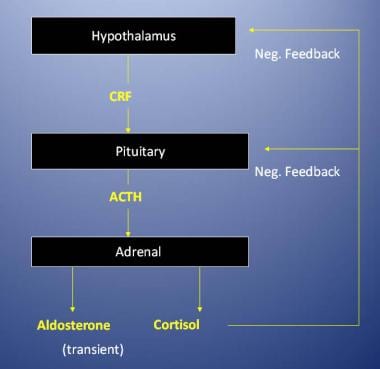
Although it is thought by experts that more than 50 steroids are produced within the adrenal cortex, cortisol and aldosterone are by far the most abundant and physiologically active. Regulation of the adrenal cortex is illustrated in the image below.
- glucocorticoids (cortisol),
- mineralocorticoids (aldosterone, 11-deoxycorticosterone), and
- androgens (dehydroepiandrosterone).
Cortisol enhances gluconeogenesis and provides substrate through proteolysis, protein synthesis inhibition, fatty acid mobilization, and enhanced hepatic amino acid uptake. Cortisol indirectly induces insulin secretion to counterbalance hyperglycemia but also decreases insulin sensitivity. Cortisol exercises a significant anti-inflammatory effect by stabilizing lysosomes, reducing leukocytic responses, and blocking cytokine production. Phagocytic activity is preserved, but cell-mediated immunity is diminished, in situations of cortisol deficiency. Finally, cortisol facilitates free-water clearance, enhances appetite, and suppresses adrenocorticotropic hormone (ACTH) synthesis.
Aldosterone is released in response to angiotensin II stimulation via the renin-angiotensin-aldosterone system,hyperkalemia, hyponatremia, and dopamine antagonists. Its effect on its primary target organ, the kidney, is to promote reabsorption of sodium and secretion of potassium and hydrogen. The mechanism of action is unclear; an increase in the sodium- and potassium-activated adenosine triphosphatase (Na+/K+ ATPase) enzyme responsible for sodium transport, as well as increased carbonic anhydrase activity, has been suggested. The net effect is to increase intravascular volume. The renin-angiotensin-aldosterone system is unaffected by exogenous glucocorticoids, and ACTH deficiency has a relatively minor effect on aldosterone levels.
Adrenocortical hormone deficiency results in the reverse of these hormonal effects, producing the clinical findings of adrenal crisis.
Adrenal medullae normally secrete 80% epinephrine and 20% norepinephrine. Sympathetic stimulation results in secretion.
Physiologic effects of glucocorticoids
Glucocorticoids are nonspecific cardiac stimulants that activate release of vasoactive substances. In the absence of corticosteroids, stress results in hypotension, shock, and death. Glucocorticoids act as follows to:- Stimulate gluconeogenesis and decrease cellular glucose use
- Mobilize amino acids and fatty acids
- Inhibit the effects of insulin
- Give rise to ketone bodies in metabolism (ketogenesis)
- Elevate RBC and platelet levels
- Exhibit anti-inflammatory effects, including the following:
- Maintenance of normal vascular response to vasoconstrictors
- Opposition to increases in capillary permeability
- Inhibition of interleukin-2 (IL-2) production by macrophages
- Stimulation of polymorphonuclear neutrophil (PMN) leukocytosis
- Reduction of adherence of macrophages to endothelium
- Depletion of circulating eosinophils and lymphocytes
- Reduction of circulating lymphocytes (primarily T cells)
- Physiologic effects of aldosterone
The primary actions of aldosterone cause the kidneys, gut, and salivary/sweat glands to affect electrolyte balance. The primary targets are the kidneys; where it stimulates reabsorption of sodium and secretion of potassium and hydrogen ions. The kidneys' effect on sodium and potassium depend on the intake of these cations (ie, increased sodium intake = increased potassium secretion). The effects on hydrogen probably can occur independently.
Persistent aldosterone excess results in atrial natriuretic factor release and renal hemodynamic changes for compensation. Congestive heart failure (CHF) and cirrhosis with ascites are exceptions that cause progressive sodium retention. Excess aldosterone results in sodium retention, hypokalemia, and alkalosis. Aldosterone deficiency results in sodium loss, hyperkalemia, and acidosis. Hyperkalemia stimulates aldosterone release to improve potassium excretion. Aldosterone is the first-line defense against hyperkalemia.
Primary adrenal insufficiency
Primary adrenal insufficiency, which can be acute or chronic, may be caused by the anatomic destruction of the gland. This destruction can have various causes, including tuberculosis or fungal infection, other diseases infiltrating the adrenal glands, and hemorrhage. However, the most frequent cause is idiopathic atrophy, which is probably autoimmune in origin.Primary adrenal insufficiency also may be caused by metabolic failure (eg, insufficient hormone production). This failure may be a result of congenital adrenal hyperplasia, enzyme inhibitors (eg, metyrapone), or cytotoxic agents (eg, mitotane).
Primary adrenocortical insufficiency is rare and occurs at any age. The male-to-female ratio is 1:1.
Secondary adrenal insufficiency
Secondary adrenal insufficiency may be caused by hypopituitarism due to hypothalamic-pituitary disease or may result from suppression of the hypothalamic-pituitary axis by exogenous steroids or endogenous steroids (ie, tumor).Secondary adrenocortical insufficiency is relatively common. Extensive therapeutic use of steroids has greatly contributed to increased incidence.
Acute adrenocortical insufficiency
Adrenal crisis may result from an acute exacerbation of chronic insufficiency , usually caused by sepsis or surgical stress. Acute adrenal insufficiency also can be caused by adrenal hemorrhage (eg, usually septicemia-induced Waterhouse-Friderichsen syndrome [fulminant meningococcemia]) and anticoagulation complications. Steroid withdrawal is the most common cause of acute adrenocortical insufficiency and almost exclusively causes a glucocorticoid deficiency.
The important elements in the history of patients with adrenal crisis or adrenal insufficiency :
- Weakness (99%)
- Pigmentation of skin (98%)
- Weight loss (97%)
- Abdominal pain (34%)
- Salt craving (22%)
- Diarrhea (20%)
- Constipation (19%)
- Syncope (16%)
- Vitiligo (9%)
Treatment
- Administration of glucocorticoids in supraphysiologic or stress doses is the only definitive therapy.
- Dexamethasone does not interfere with serum cortisol assay and, thus, may be the initial drug of choice. However, because dexamethasone has little mineralocorticoid activity, fluid and electrolyte replacement are essential.
- A short ACTH stimulation test may be performed during resuscitation. Once complete, hydrocortisone 100 mg IV every 6 hours is the preferred treatment to provide mineralocorticoid support.
- Delaying glucocorticoid replacement therapy while awaiting the results of the ACTH stimulation test is inappropriate and dangerous.
- In addition to corticosteroid replacement, aggressive fluid replacement with 5% or 10% intravenous dextrose and saline solutions and treatment of hyperkalemia is mandatory. Fludrocortisone, a mineralocorticoid, may also be given.
- A thorough search for a precipitating cause and administration of empiric antibiotics is indicated. Reversal of coagulopathy should be attempted with fresh frozen plasma.
- Pressors (eg, dopamine, norepinephrine) may be necessary to combat hypotension.
There is a lot of information available on this subject. Excellent article. If you are a gamer, you should improve your clicking speed so that you can read this profile about Kohi click test and increase click speed.
ReplyDelete